
Stopping the Loss of Rural Healthcare Services
Thursday, November 21 is National Rural Health Day, and the news about rural health isn't good. Working-age people living in rural areas are 43% more likely to die from natural causes than in urban areas. Over the past 20 years, the death rate for working-age adults living in rural areas increased, while mortality decreased for those in urban areas.
Many of these deaths occur for preventable reasons. For example:
- Pregnancy-related deaths are 60% higher in rural areas than in urban areas.
- Deaths from heart disease are 45% higher in rural areas than urban areas for working-age men and 69% higher for working-age women. While deaths from heart disease decreased in urban areas over the last two decades thanks to improved prevention and treatment, working-age women in rural areas are more likely to die from heart disease now than 20 years ago.
- While cancer-related death rates for working-age people have decreased in both urban and rural areas thanks to improved prevention, screening, and treatment, the death rate in rural areas is 27-31% higher than in urban areas.
One of the reasons for this disparity is the lack of healthcare services in rural areas. Nearly 200 rural hospitals have closed over the past two decades, leaving millions of rural Americans without access to emergency care, inpatient care, and preventive care services that people in the rest of the country take for granted.
More Rural Healthcare Services Are Lost Every Year
More rural communities are losing healthcare services every year. In just the past two years:
- More than 50 rural hospitals have eliminated labor and delivery services, forcing thousands of mothers to travel long distances to obtain prenatal care and to deliver their babies. More than half of the rural hospitals in the U.S. no longer offer labor and delivery services.
- Over 30 rural hospitals have eliminated inpatient services, forcing thousands of seriously ill individuals in those communities to be transferred to a hospital far from home in order to receive the services they need.
- 14 rural hospitals have closed entirely, forcing the residents of most of those communities to travel long distances for both emergency care and preventive care services.
The Primary Cause: Underpayment by Private Insurance Companies
What is causing the loss of rural healthcare services? In most cases, the biggest reason is that health insurance plans pay rural hospitals less than what it costs to deliver essential services such as emergency room visits, labor and delivery, and primary care.
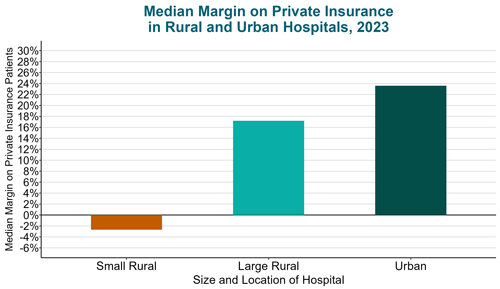
Contrary to popular belief, the biggest problem for small rural hospitals is not low payments from Medicare and Medicaid, but low payments from private health insurance companies, both commercial insurance plans and Medicare Advantage plans. Large hospitals, both in urban and rural areas, make high profits on patients with private insurance that enable them to offset losses on uninsured patients and low payments from Medicaid programs. In contrast, the majority of small rural hospitals lose money on patients with private insurance.
Similarly, it is often assumed that low Medicaid payments are the reasons hospitals lose money on maternity services, but over 40% of births in rural communities are paid for by private health plans, so inadequate payments from private payers also threaten the viability of rural maternity care.
A Growing Problem: Underpayment by Medicare Advantage Plans
Traditional Medicare pays higher amounts to small rural hospitals than to larger hospitals because the fixed costs of delivering essential services results in higher costs per patient in small communities than in larger areas. Medicare Advantage (MA) plans, however, are not required to pay the same amounts as Traditional Medicare.
Small rural hospitals report that they lose large amounts of money on Medicare Advantage patients because the MA plans either pay them less than Traditional Medicare, deny claims at a high rate, or both. Because more and more Medicare beneficiaries have been enrolling in MA plans every year, small rural hospitals have been losing more and more money every year.
More Services Will Be Lost Without Immediate Action
More than 700 rural hospitals – over 30% of all rural hospitals in the country – are at risk of closing because of the serious financial problems they are experiencing. Over half of these hospitals are at immediate risk and could close within the next 2-3 years unless their finances improve significantly.
Long before hospitals close, they will be forced to eliminate services that are important to their communities. Almost 40% of the rural hospitals that still have labor & delivery services – over 300 hospitals – lost money on patient services overall in 2023, so their ability to continue delivering maternity care is at risk.
What is Needed
Requiring Adequate Payments for Essential Services
In order to ensure rural communities have essential healthcare services, private health insurance companies (including Medicare Advantage plans) have to pay rural hospitals and clinics enough to cover the cost of delivering essential services in their communities. It does little good to have health insurance if there is nowhere to use it because the local hospital and/or physician practices have been forced to close.
Unfortunately, health insurance companies are unlikely to pay adequately unless regulators require it or the health plans' customers demand it:
- Employers should choose health plans for their employees based on whether the plans pay the local hospital, physicians, and other providers adequately and appropriately, not just based on whether the premiums or administrative fees are lower than other insurance companies charge. The Purchaser Business Group on Health recently adopted standards for how health insurance plans should pay for maternity care services; all employers (including federal, state, and local government employers as well as private businesses) should use these standards. Similar standards should be established for emergency and primary care in rural areas.
- Congress and the Centers for Medicare and Medicaid Services (CMS) should require that Medicare Advantage plans pay small rural hospitals adequately for their services. In addition, MA plans should be required to pay rural hospitals in a timely way; the high rates of claim denials and long delays in authorization of services by many plans are harming both patients and small hospitals.
Using Standby Capacity Payments for Essential Services
The financial problems at small rural hospitals are caused not only by the inadequate amounts they are paid for services, but also by the problematic method all payers use to pay for services.
- The physicians and nurses in a rural emergency room must be standing by 24 hours a day, ready to provide emergency care, but they are only paid when they actually treat a patient. As a result, while it is good for patients when there are fewer emergencies, it creates a loss for the hospital and physicians.
- Similarly, in order to offer labor and delivery services, a small hospital needs to have physicians and nurses ready to deliver a baby all day, every day, even though there may be no deliveries at all on many days. However, the hospital and clinicians are only paid when there is a delivery, so fewer pregnancies means the hospital and clinicians will lose money.
In order to ensure a rural hospital has adequate revenues to support the fixed cost of this standby capacity, the hospital needs to receive Standby Capacity Payments from both private and public insurance plans, in addition to being paid Service-Based Fees that cover the variable costs of individual services. More details on this approach are available in CHQPR's report A Better Way to Pay Rural Hospitals.
For More Information
Detailed data about individual hospitals, the causes of rural hospital problems, and the solutions needed to address them are available at RuralHospitals.org.
Rural Hospitals at Risk of Closing includes a state-by-state list of:
- the number of rural hospitals that have:
- closed completely within the past decade, or
- closed inpatient services and converted to a “Rural Emergency Hospital”;
- the percentage of the open inpatient hospitals that:
- lost money on patient services during the most recent year available,
- are at risk of closing because they have been experiencing losses over multiple years,
- are at immediate risk of closing (i.e., within the next 2-3 years) because of the size of the losses they have experienced and the lack of assets to cover those losses.
Addressing the Crisis in Rural Maternity Care includes a state-by-state list of the number and percentage of rural hospitals that no longer deliver babies and the distance to the closest hospital that does deliver babies. The list also shows how many of the remaining rural maternity hospitals have been losing money overall.